The Common Vein Copyirhgt 2010
Definition
Menorrhagia is excessive bleeding at menses with multiple causes.
The most common causes of menorrhagia are benign uterine polyps or fibroids. However, menorrhagia may also have more serious causes including bleeding disorders or uterine cancers.
The result is a prolonged period of menstruation (>7 days) or excessive blood flow at menses (>80 cc/cycle).
Structural changes vary depending on cause.
Functional changes also vary with cause, but always include excessive bleeding, giving women their common clinical presentation. Women with menorrhagia often describe soaking through a menstrual pad every hour during menses.
Diagnosis is based on clinical history and treatment depends on the cause found at evaluation.
Endometrial Filling Defect – Polyp or Submucosal Fibroid |
|
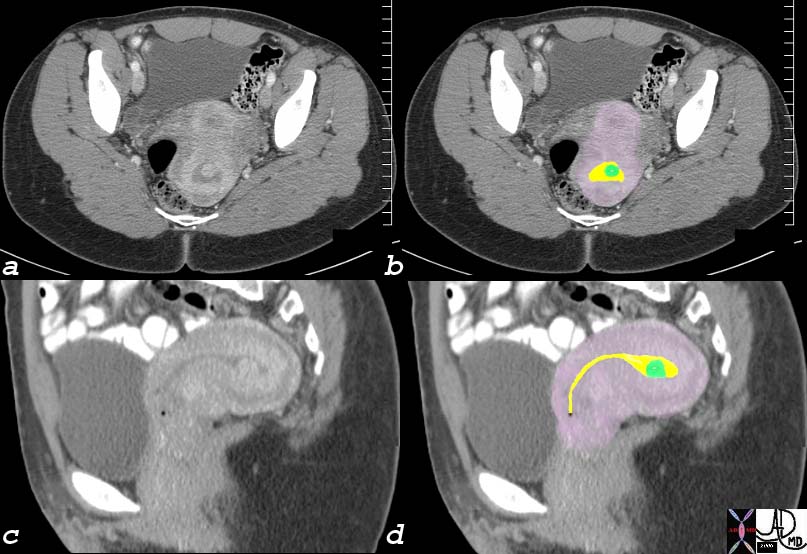
The coronal reconstruction of a CTscan of a young woman shows a retroverted uterus with a enhancing filling defect (green overlay in b) in the endometrial cavity (yellow). These findings are consistent with either an endometrial polyp or a submucosal fibroid. Endometrial carcinoma is a remote possibility. endometrial fluid = yellow polyp = green myometrium = pink Image Courtesy Ashley Davidoff MD Copyright 2010 76018c01 |
|
Submucosal Fibroid |
| The USscan (sonohysterogram) scan is from a 41year old female, who presents with dysfunctional uterine bleeding. The study reveals a 4mms submucosal nodule shown at pathology to be a submucosal fibroid.
Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 84299c041.8 |
|
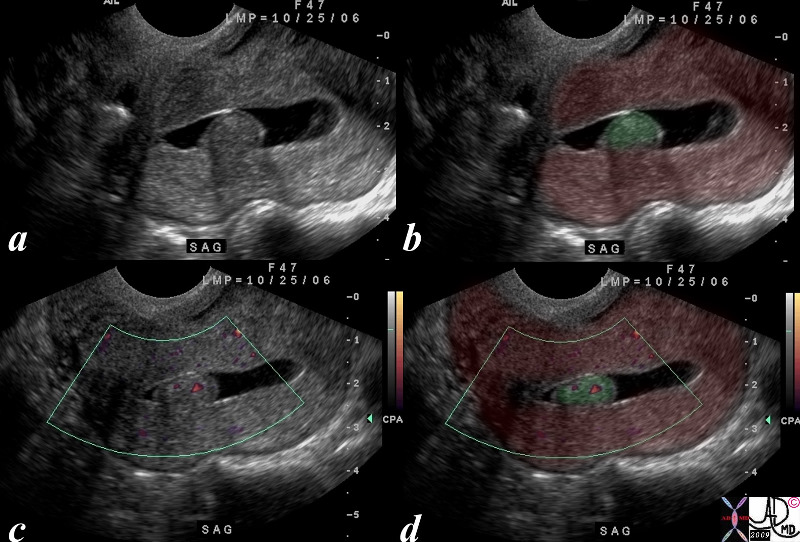
Hyperplastic Polyp |
| The USscan (hysterosonogram is from a 47year old female, with history metrorhagia dysfunctional uterine bleeding. The studies reveal a mass in the uterus within the endometrial cavity The polypwas shown to be a benign hyperplastic polyp. uterus endometrium mass polyp hyperplastic USscan hysterosonogram
Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 84299c05.8s |
|
Filling Defect |
|
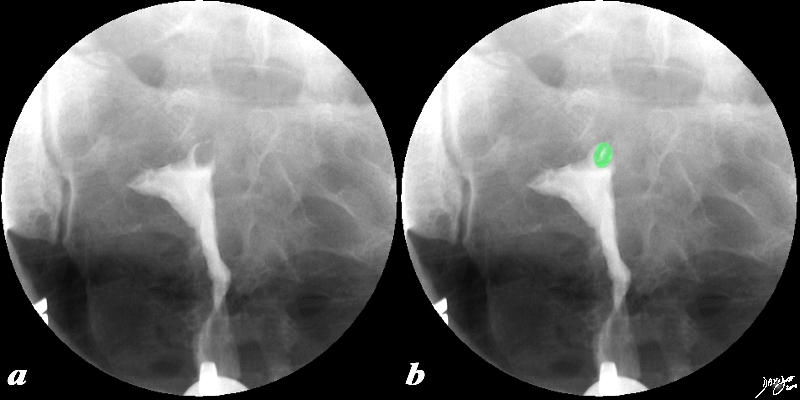
This 38 year old female presents with a history of infertility. The hysterosalpingogram shows non filling of both Fallopian tubes and a filling defect (green) in the region of the patient’s left cornu that likely is the cause of the obstructed left tube and in part the cause of the infertility. The lesion is most likely a submucosal fibroid. Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 96897c02.8s |
|
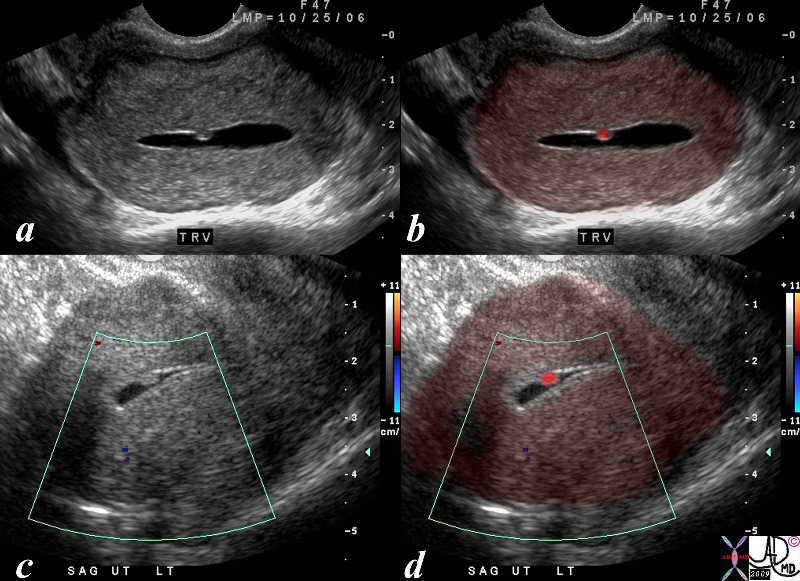
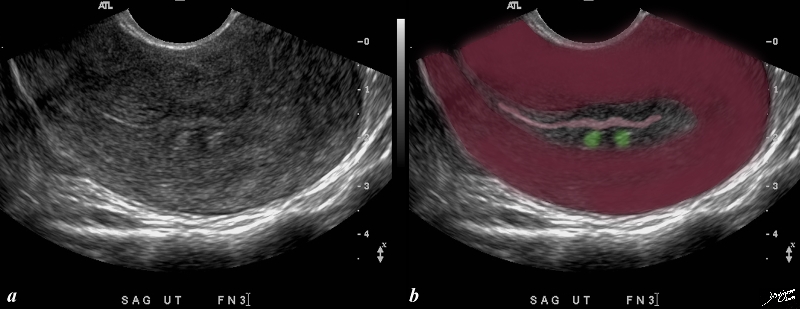
Two Lesions in the Junctional Zone Impinging on the Endometrium |
| This patient presents with menorrhagia. Two echogenic nodules (overlaid in green) are seen in the subendometrial layer, (junctional zone). They are in close proximity and do appear to have appositional relationships with the endometrial stripe. They appear to and distort the endometrial lining. These findings could account for the patient’s menorrhagia. Note that the uterus is retroverted Included in the differential diagnosis are submucosal fibroids, and dystrophic changes in prior foci of adenomyosis. An MRI would be helpful in further characterizing these lesions in the subendometrial layer
copyright 2009 all rights resrved Courtesy Ashley Davidoff MD 85641bc01.8s |
|
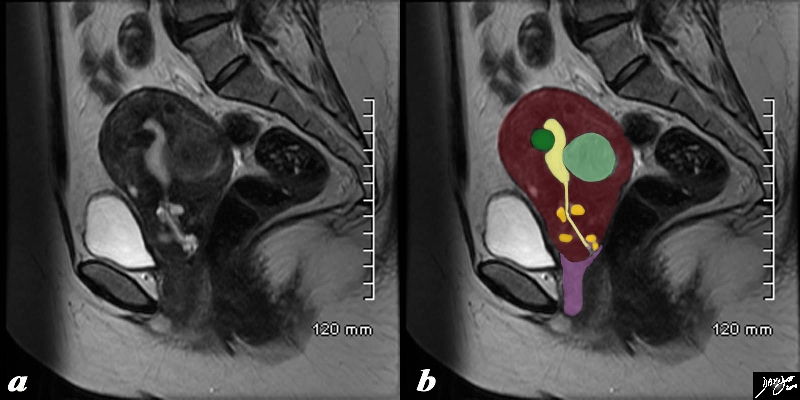
Fibroid Impingement on the Endometrium |
|
In this sagittal view of a T2 weighted MRI of the uterus of a 42 year old female with multiple fibroids two of which impinge on the endometrial cavity (the larger (light green) from posterior and the smaller (dark green) from anterior resulting in a sigmoid shaped cavity (yellow). In addition incidentally noted Nabothian cysts (orange) are seen within the cervix. Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 96531c02.8s |