
Copyright 2008
Definition
Adenomyosis is a disease of the myometrium caused by misplaced or ectopic endometrium in the myometrium resulting in myometrial hyperplasia and smooth musce hypertrophy clinically manifesting as pelvic pain and uterine enlargement. The entity can be focal or diffuse
The exact cause of the displacement is not known but it is presumed that a breach in the endometrial myometrial barrier enables a small amount of endometrium to translocate and remain viable. There is a high prevalence rate with about 40% of hysterectomy specimens displaying the entity.
Clinically the patient presents with dysmenorrhea and menorrhagia and on exam the uterus is enlarged.
The diagnosis is best made by MRI which shows a thickened junctional zone (>10-12mms) of the uterus The deposition of acute blood, blood degradation products such as iron, or the the presence of fluid filled microglandular deposits in the junctional zone make the MRI findings highly specific for the diagnosis.
Treatment options include pain management with NSAIDS, hormonal manipulation. Surgery and hysterectomy is the only current option for cure.
Adenomyosis Diffuse or focalHystero – looks like pseudoodiverticuliThickening of jnal zone.12mmHigh focal T2 cysts incomplete
Imaging
MRI
Imaging study of choice is MRI and the most helpful sequence is T2 weighted which shows the hypointense junctional zone sanwiched between the hyperintenseendometrial cavity and the slightly hyperintense outer myometrial layer.
Thickening of the Junctional Zone
The junctional zone thickening is key to the diagnosis The junctional zone normally measures 8mm or less. Between 8-11mm it is considered indeterminate, and when it measures greater than 11mm it is considered diagnostic for the disease.
The junctional zone may thicken normally in the first few days of the menstrual cycle or during myometrial contractions.
Heterogeneity in the Junctional Zone
Cystic changes in the junctional zone are characteristic and relatively common and represent small blood blisters.
Linear striations radiating from endometrium to myometrium are also seen but these are not as easy to discern. These probably reflect a breech in the endometrium with the microscopic tear extending into the myometrium.
Hysterosalpingogram
HSG shows linear contrast streaking from the endometrium into the junctional zone associated with punctuate collections likely representing the small cystic regions identified on MRI
|
Thickened Junctional Zone |
| This T2 weighted MRI of a 41 year old female shows thickened junctional zone of the uterus measuring up to 12 mms characteristic of adenomyosis
83298c.81s uterus junctional zone thickened enlarged MRI T2 weighted Adenomyosis the uterus Courrtesy Ashey Davidoff MD copyright 2009 ectopic tissue |

|
Thickened Junctional Zone |
| This T2 weighted MRI of a 41 year old female shows thickened junctional zone of the uterus measuring up to 12 mms characteristic of adenomyosis
83296.8s uterus junctional zone thickened enlarged MRI T2 weighted Adenomyosis the uterus Courrtesy Ashey Davidoff MD copyright 2009 ectopic tissue |

|
Adenomyosis Thickened Junctional Zone Enlarged Uterus |
| This T2 weighted MRI of a 41 year old female shows thickened junctional zone (light maroon) of the uterus measuring up to 12 mms characteristic of adenomyosis
code uterus junctional zone thickened enlarged MRI T2 weighted Adenomyosis the uterus Courrtesy Ashey Davidoff MD copyright 2009 |

14707c01.8s
|
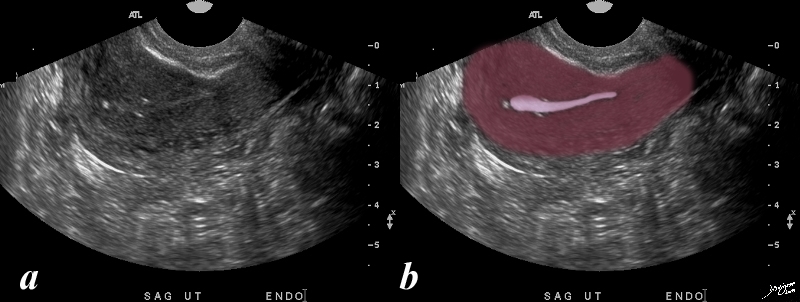
Dystrophic Calcification in Subendometrial Region |
| 37 year female with calcifications along the endometrial cavity
uterus ultrasound USscan Courtesy Ashley Davidoff Copyright 2009 all rights reserved 83543c.83s |
|
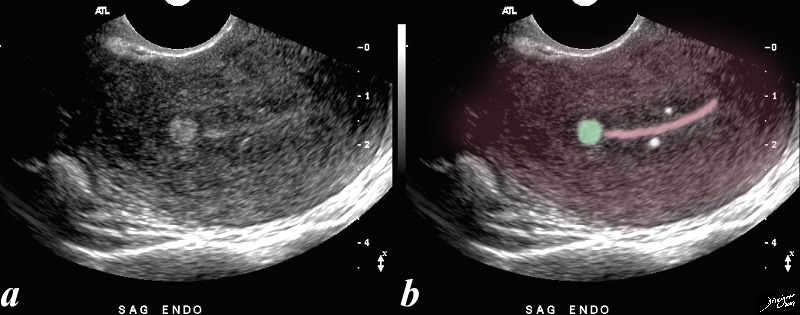
Dystrophic Calcification in Subendometrial Region |
| 52 year-old patient presents with menorrhagia. Two punctate echogenic nodule are in the subendometrial junctional zone, (overlaid in white in b) that are thought to represent dystrophic areas of calcification in prior foci of adenomyosis. The larger echogenic focus (green) was shown to be a benign hyperplastic polyp by pathology after a D and C. The polyp probably accounted for the patient’s menorrhagia. Note that the uterus is retroverted
Courtesy Ashley DAvidoff copyright 2009 all rights reserved 85641b01c.81s |
References
Ken Tamai, MD, Kaori Togashi, MD, Tsuyoshi Ito, MD, Nobuko Morisawa, MD, Toshitaka Fujiwara, MD and Takashi Koyama, MD
MR Imaging Findings of Adenomyosis: Correlation with Histopathologic Features and Diagnostic Pitfalls1 RadioGraphics January 2005, 25, 21-40.