
Copyright 2009
Definition
Endometriosis is a disease of the endometrial lining caused by misplaced or ectopic endometrial tissues that are located beyond the uterus and usually results in pelvic pain.
It occurs in 5-10% of women. When endometrial tissue is located outside of the uterus, it can cause pelvic and back pain as well as dyspareunia. The potential of endometrial tissue to be deneuded into the peritoneal cavity is based on the connection of the cavity with the peritoneal space via the fallopian tubes.
From a structural standpoint, endometriosis ranges in size from small microscopic implants, are commonly about 1-2cms in size but can develop into endometriomas that may be up to 5-6cms in size. They are often round in shape much like a blood blister (aka endometrioma) after they have bled, but they often induce reactive fibrotic changes in which case their shape takes on a linear or plaque like form.
The most common site of involvement is the ovaries but endometriosis also can affect the broad ligaments, fallopian tubes, uterosacral ligaments, cul de sac, or other locations in the pelvis or abdomen, including the ureters and the bowel serosa. Endometriosis is rarely more far reaching including the kidneys, brain, diaphragm, and pleura. When it involves the iaphragm or pleura, shoulder pain may be associated with the entity. Catamenial pneumothorax is pneumothorax induced by the menstrual cycle and implies endometriosis of the pleura.
The nodules can be red-blue to yellow-brown in color, (chocolate cysts) occur just below the serosa of the organ to which they are attached. As the lesions undergo recurrent hemorrhage, they can become associated with fibrosis a stated.
Rarely they may be associated with malignant transformation.(<1%)
Clinically the entity more commonly occurs in nulliparous women and the degree of pain is variable. As endometrial tissue, it is responsive to the cyclical hormonal fluxes, and thus may bleed in response to hormonal changes. Pain commonly occurs at the time of the menses. The volume of ectopic endometrial tissue does not correlate with the severity of the pain, but rather with the depth of infiltration into the tissue, or the degree of distension that might occur. The pain is usually recurring and commonly but not necessarily occurs during the menses. With induction of fibrosis, pain may be caused by other structural changes that are unrelated to the menses.
Diagnosis is suspected clinically and confirmed by ultrasound. If ultrasound is negative MRI may be helpful, laparoscopy is indicated both for diagnosis of small or flat lesions lesions as well as for thrapy. Endometriomas have a characteristic appearance. Microscopic deposits which may cause symptoms may not be identified by imaging techniques and may only be seen laparoscopically.
Treatment options depend on patient preference, including whether fertility is desired, but include both medical and surgical options. Medical management frequently involves suppression of regular menses/hormones and surgical options typically attempt to remove endometrial tissue or surgical menopause (i.e. oophorectomy and hysterectomy).
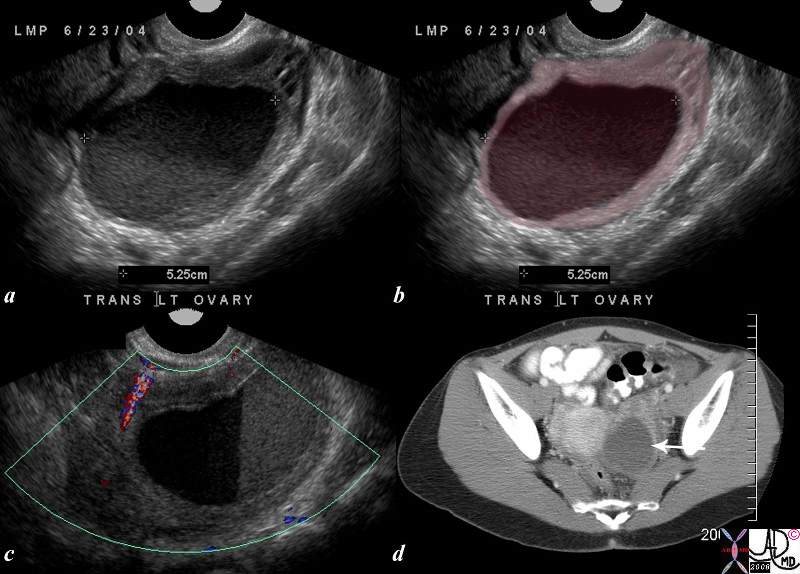
25 year old female presents with painful menses. The ultrasound shows a cystic mass in the pelvis with a large amount of debris in the cystic cavity consistent with a chocolate cyst. Although the appearance is consistent with endometriosis, a hemorrhagic cysts is possible and the distinction may only be made pathologically
uterus pain ovary hemorrhagic cyst endometrioma 83261c01.8s
Ashley Davidoff MD
Adenomyosis
|
Thickened Junctional Zone |
| This T2 weighted MRI of a 41 year old female shows thickened junctional zone of the uterus measuring up to 12 mms characteristic of adenomyosis
83298c.81s uterus junctional zone thickened enlarged MRI T2 weighted Adenomyosis the uterus Courtesy Ashley Davidoff MD copyright 2009 ectopic tissue |

|
Thickened Junctional Zone |
| This T2 weighted MRI of a 41 year old female shows thickened junctional zone of the uterus measuring up to 12 mms characteristic of adenomyosis
83296.8s Courtesy Ashley Davidoff MD copyright 2009 ectopic tissue |

|
Adenomyosis Thickened Junctional Zone Enlarged Uterus |
| This T2 weighted MRI of a 41 year old female shows thickened junctional zone (light maroon) of the uterus measuring up to 12 mms characteristic of adenomyosis
Courtesy Ashley Davidoff MD copyright 2010 |

Adenomyosis vs Submucosal Fibroids |
|
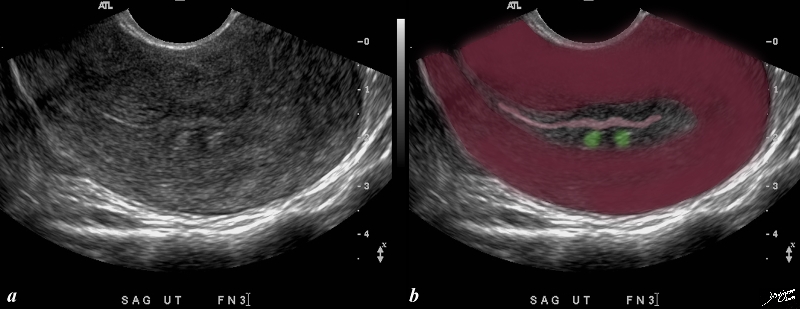
This patient presents with menorrhagia. Two echogenic nodules (overlaid in green) are seen in the subendometrial layer, (junctional zone). They are in close proximity and do appear to have appositional relationships with the endometrial stripe. They appear to and distort the endometrial lining. These findings could account for the patient’s menorrhagia. Note that the uterus is retroverted Included in the differential diagnosis are submucosal fibroids, and dystrophic changes in prior foci of adenomyosis. An MRI would be helpful in further characterizing these lesions in the subendometrial layer Copyright 2009 all rights reserved Courtesy Ashley Davidoff MD 85641bc01.8s |
Remote Adenomyosis |
|
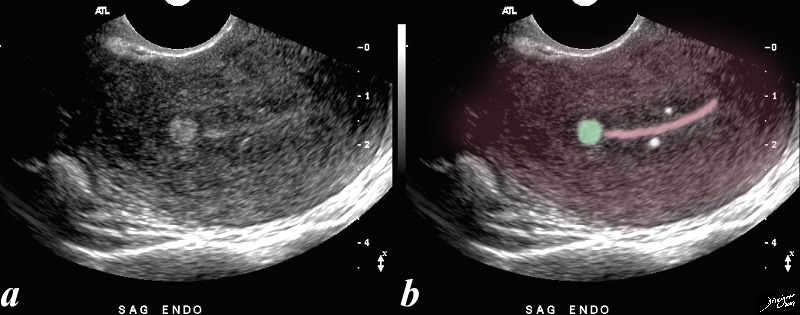
52 year-old patient presents with menorrhagia. Two punctate echogenic nodule are in the subendometrial junctional zone, (overlaid in white in b) that are thought to represent dystrophic areas of calcification in prior foci of adenomyosis. The larger echogenic focus (green) was shown to be a benign hyperplastic polyp by pathology after a D and C. The polyp probably accounted for the patient’s menorrhagia. Courtesy Ashley DAvidoff copyright 2009 all rights reserved 85641b01c.81s |
Cause
Proposed pathophysiological theories include
Metastatic seeding:
This theory proposes retrograde menstruation, with spillage into the peritoneum, transvascular spread,or implantation into the myometrium. The cells retain their properties a sviable endometrium and are subject to the hormonal changes fluxes
Metaplastic theory:
Since the endometrium and the peritoneal lining originate from the same coelomic epithelium may undergo metaplasia and and develop into endometrial tissue
Induction theory
Shedding of substances by the endometrium that induce the formation of of endometrium from undifferentiated mesenchymal tissue.
Diagnosis
Ultrasound for pelvic pain is the study of choice for pelvic pain, but laparoscopy is necessary when there is high level of clinical suspicion for its diagnostic and therapeutic capabilities;
Direct visualization of all types of lesions
Can treat or biopsy
Disadvantage invasive
May be limited by adhesions
US
Good for ovarian detection and characterization
Difficulty with peritoneal implants
Findings include large ovarian cystic lesions with complex sepations, low level internal echoes, no flow in the cyst or septations
MRI
High specificity 90% sensitivity 90%
Good for monitoring response to therapy
Hard to see non pigmented nodules and adhesions
T1 axial sagittal
T2 axial 3.5mm cuts
T1 fat sat axial sagittal coronal
4mm for hemorrhagic lesions
T1 gad if neoplasm suspected otherwise not usually used
T1 bright with no loss of signal on fat sat
Sometimes heterogeneous due to degraded products
Some ;arger lesions show septations
T2 signal variable with “shading” thought to be due to repeated cycles of hemorrhage Hemosiderin in the wall leads to loss of signal in the wall on T1 and T2